In this issue: A simple drink that changed the world, a brief response to an article about Andrew Huberman, and some live events I’ll be inflicting upon the world
Three fingers pinch labon (salt), a hand scoop gur (raw sugar) and 500ml good water
I read an article around the time I began as a doctor, which made a lasting impact on me, and recently I decided to revisit it. It was a list of the 15 greatest medical breakthroughs of the last 200 years or so. I thought it might make a fun video to go through the list, but having made a video about one of the items specifically, I suspect it will be more logical and less frenetic to make dedicated short videos about each point, lest it be a rather rushed affair.
The fact that I jumped the gun was a bit of over-excitement at reading about a story with a personal connection, not only in terms of the geography, but the people themselves. One of the 15 greatest medical breakthroughs was oral rehydration therapy, pioneered in Calcutta (Kolkata) and Dacca (Dhaka). A deceptively simple combination of water, salts (to replace lost electrolytes), and sugar (to take advantage of the gut’s sodium glucose transport proteins*).
Thanks for reading The Medlife Monthly(ish)! Look, two issues in a calendar year! Sure fire sign this newsletter has ascended into a must-read, so why not subscribe? ALL HAIL TRISOLARIS
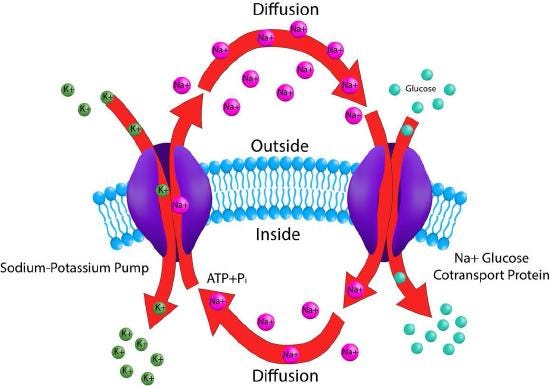
*If you’re interested in sodium glucose transport proteins (and who wouldn’t be?!), biochemist Robert Crane discovered the first example of biological co-transport (flux coupling) in 1960, the phenomenon where two molecules are transported across a membrane, typically without requiring ATP. He described the sodium glucose linked transport (SGLT) as the mechanism by which the body absorbs glucose in the intestines, which directly led to the invention of oral rehydration therapy, as the presence of both salt and sugar makes use of these cotransporters to maximise absorption.
The Na+/K+ ATPase (left) and sodium/glucose pump (right). In normal physiology, the sodium gradient generated by the Na+/K+ ATPase is used by the sodium/glucose pump to import glucose into the cell. These are known as antiporters (carrying against) and symporters (carrying together) respectively.
Knowledge of SGLT directly led to a therapy designed to maximise absorption of sugar and salt, but in a wonderful example of how understanding a mechanism can act as a springboard for further research, decades later this same cotransporter would once again hit the headlines, although this time being used to treat almost the opposite problem. SGLT2 inhibitors are a class of medication I prescribe on almost a daily basis. Initially developed as a diabetic medication, they have become mainstays of cardiovascular care.
If recruiting SGLT helps increase body glucose, inhibiting it should do the opposite. By targeting SGLT2, found in the kidney, drugs like dapagliflozin or empagliflozin, prevent (re)absorption of glucose. In other words, they make diabetics piss out more sugar, lowering blood sugar and also explaining why patients can report more urinary tract infections.
You may be aware that drugs have a patent period of 20 years, however often the first few years are taken up with testing and trials, meaning it comes to the market with significantly less than twenty years to turn a profit. The SGLT2 inhibitors were doing a solid trade as diabetic drugs, before some trial data emerged showing that they reduced cardiovascular mortality and boom, cardiology baby. The mother lode! Make it raaiiinn! I imagine this is how Pharma execs talk, who knows.
Cardiology is where the money is, but they only had 7 years left on the clock. Cue the last few years of heavy promotion and rebranding, pivoting from wooing diabetologists (nerdy, wear tweed, bookish, ride a penny farthing bicycle) to pursuing cardiologists (giga chads, wear the hides of vanquished foes, manipulate time, ride lasers). Joking aside, the data are clear – they are very effective for the right patients. The fact it took a few decades from the initial SGLT discovery to this medication can be seen as breathtakingly fast or glacially slow, depending on your point of view.
I’m quite enjoying these shorter videos with simpler production, but without a script I do forget things. One thing I meant to mention was that none of the people involved attempted to patent oral rehydration therapy, reminiscent of Jonas Salk’s famous retort to an inquiry about whether he planned to patent the polio vaccine, “could you patent the sun?” For further reading on how my glib throwaway reference is actually much more complex, this was interesting.
Nevertheless, it felt like an attitude from a bygone age. Now experts frequently seek self enrichment. I am reluctant to criticise that, as scientists are, on average, grossly underpaid for how much utility they can bring into the world, and I enjoy people being successful, but it does draw a stark comparison between humble professionals like Dilip Mahalanabis, working in refugee camps on research salaries, developing treatments that could save millions; and the most visible scientists of our present day.
Hubris, man
In spite of working scientists and doctors influencing peoples’ lives in the most profound way imaginable, we literally use the term influencer to refer to these modern science personalities. Perhaps the most famous health influencer in the world today is Andrew Huberman, whom I have mentioned in a few videos already, and always with the same criticism – his fundamental lack of ability to appraise clinical science. There are many more criticisms to be made, such as financial conflicts of interest or failing to challenge guests’ false claims, but the fact he, or his team, clearly do not understand the clinical research they read, is such a fundamental flaw that it trumps everything else. I have no doubt he is highly accomplished in the specific field of retinal signalling he specialises in professionally, but this is as far from a clinical trial as the Large Hadron Collider, and yet his public persona is that of a health influencer, rather than a retinal neurobiologist. TIME Magazine last year called him the man who got America to “care about science”, and perhaps what is most frustrating is the idea that people perceive the things he says to be science. If anything, ‘science cosplay’ would be a closer approximation to the truth. If you are looking for more in-depth analysis as to why I say this, I promise I will have a lengthy dissection out in a few weeks. Please don’t ask for clarification about what is implied by the word ‘few’. Or ‘weeks’.
Millions more people have heard of Andrew Huberman than Dilip Mahalanabis. That’s a trite observation, and I guarantee 99% of working scientists have no interest in fame. But I couldn’t help making the comparison this week, as an article about Huberman was recently published in the New York Magazine, and about four hundred people sent it my way, as I’ve been a vocal critic of the content of Huberman’s podcast for several years, hence I wanted to briefly comment on it. Funnily enough there is a connection between the two stories in this email.
Scott Carney is an author and a friend, whose books ‘The Red Market’ and ‘What Doesn’t Kill Us’ were the starting points for my videos about buying human remains, and the Wim Hof technique, respectively. He recently published ‘The Vortex’, about the devastating 1970 Bhola Cyclone, which claimed half a million lives and acted as the backdrop not only to Mahalanabis and colleagues’ groundbreaking discoveries about oral rehydration therapy, but also war, genocide, famine, revolution, and liberation. Even with George Harrison corralling friends into the Concert for Bangladesh, I feel this chapter in 20th century history is still sorely un-taught and unknown outside South Asia (NB extremely upsetting reading).
My father was working for Oxfam and heavily involved in relief efforts at the time, so I put Scott in touch with him for The Vortex. And strangely enough, Scott is one of the quoted parties in the recent Andrew Huberman article, which is a coincidence that I’m sure no one else finds particularly amusing, but if I’m going to be taken seriously as a columnist, then I need to embrace the tenuous segue more than ever.
This is all to say that as I know my magnum opus (ha) video essay on medical influencers is still some weeks away, and people were clearly keen for me to comment on the Huberman article, here are my thoughts (I’m only feigning annoyance at everyone sending it to me, I actually always appreciate people sending links my way…even if many are a fairly depressing insight into the the shady world of quacks).
I don’t feel it’s my place to comment on anyone’s personal life. I wonder if separating out revelations about his relationships and so forth from a distinct article about his scientific credibility would have made for a less confused piece. Not that I am downplaying the significance of his alleged behaviour, especially to the women involved, but the article skipped between seemingly unrelated topics. There was a brief mention of Huberman’s heavy promotion of useless supplements, financial conflicts, and quite a stunning revelation that he doesn’t actually have a lab, but these were buried as footnotes among everything else. Which is a shame, because they speak directly to how reliable his scientific claims are. Furthermore, the mixing of relationship drama with professional conduct has predictably led to his fans dismissing the article as a ‘hit piece’.
I have identified what I see as the ten key problems with the modern world of medical influencers, giving particular focus to podcasters, and am attempting to flesh out the bones as soon as I humanly can, but until then please accept the above as my humble offering to the Huberman discourse. More anon.
Simplicity is key
Leaving aside the personalities involved, the most striking contrast between these two ideas I’d been mulling over recently was impact. Medical influencers recommend superfluous window dressing with little to no evidence, for people who are mostly already in good health, in a predominantly highly developed world where deficiencies that would warrant supplementation are rare. They focus an altogether undeserved amount of time on minutiae like whether blueberries are better than strawberries at maximising your glycaemic fibre sinusoidal retention curve, whether desegmented L-athionine wankidase is superior to monosyllabic pre-autotrophed decoupled D-whackendronone supplementation in the pursuit of a made-up number on a $600 smartwatch, whether 8.3 minutes of UV-B 400nm invisible refracted reflected visible diffracted moonlight is better than 8.4, or droning on for 3 hours about how to fucking breathe, instead of reinforcing the simple message that you can achieve 90% of modifiable health benefits by really maximising the most simple of instructions. Things you’ve heard me say so many times, I feel duty-bound to apologise for in advance: eat well, sleep well, exercise frequently, reduce stress, don’t smoke, seek meaningful social interaction, choose your genes carefully. But of course, if you’re entire business model is predicated upon having something new to talk about every week, you can’t focus on that simple, high yield, easy-to-access stuff. You must convolute everything, such that people elevate you to guru status and continue to seek out your wisdom.
And meanwhile, sadly anonymous researchers, especially those working in resource-poor environments, can have an incomprehensible impact on humanity.
The common theme here is that simplicity can often be the key. The reason I don’t consume medical podcasts unless researching a video is because they needlessly over-complicate things. Simplicity is key, not only in terms of results, but for your own convenience. Why burden yourself with so many additional variables, when you achieve so much with an uncomplicated set of starting instructions?
I once was blind
I valued being able share with you the story of the old school paediatric cardiologist who deliberately tore a hole in a baby’s heart in order to save their life, and I think another one can close out this newsletter with a theme of simple interventions having enormous effects. I know medics love a bit of inter-specialty banter, but secretly I love celebrating doctors that do amazing stuff. Ophthalmology as a field wasn’t one that grabbed my interest as a student, as I relished the complex mechanisms at play with critical illness, and sought a specialty with major emergencies and lots of adrenaline, but I’ve never been more blown away than when chatting to an ophthalmologist who had returned from a trip to Malawi. Envy isn’t the right word, but something close.
A fairly boring and routine operation here in the UK, cataract surgery, is hardly what gets my ophthalmology colleagues bouncing out of bed. In the UK, cataracts rarely progress that far before being treated. But in the rural hospital in Africa that he visited, where the nearest facilities for fixing a cataract are hundreds of kilometres away, and perhaps even further away financially, he could utterly transform people’s lives. An ophthalmologist can do a lens removal and implantation in a few minutes.
Can you imagine enabling someone to see? A blind woman, perhaps no longer able to see her children or grandchildren, in a village without modern aids, entered the operating theatre unable to see her hand in front of her face. Her operation was done by my colleague and a local surgeon he was training. Fifteen minutes later she walked out with a new set of lenses, to begin a new chapter in her life. Total cost of the lenses: perhaps $200. They operated on about 80 patients in a single day. I confess I wanted to know how that felt. The satisfaction you must derive from giving someone back their vision is hard to contemplate, leave aside doing it 80 times in a day. An amazing grace.
Perhaps amusing only to me, but my mother-in-law was just started on empagliflozin and here a few days later I see its mechanism of action mentioned here. I had been meaning to look up the pharmacology of the drug (it’s newer than the last time I was practicing medicine) but hadn’t gotten around to it and I guess now I don’t need to. Thanks!
Your bit on the salt/sugar drink reminded me, rather horribly, of my first nightshift at an industrial bakery when I was 18. I was put on the bread roll ovens, which radiated a phenomenal amount of heat, so by my first break, I was desperate for a drink. One of the old lags pointed out a drinks station near the ovens and I gratefully poured myself a generous glass of what I took to be lime cordial. It was, of course, not that simple - being laced with salt to replace what we lost from our profuse sweating. Much to the assembled old lags' delight, I spat the whole mouthful out in horror! It was absolutely vile - even more so because so unexpected. The old boys, some of whom had worked there for decades, drank the stuff as if it was water, but, in the two months I was there, I could never get used to it.





Great thoughts, as always.
Perhaps amusing only to me, but my mother-in-law was just started on empagliflozin and here a few days later I see its mechanism of action mentioned here. I had been meaning to look up the pharmacology of the drug (it’s newer than the last time I was practicing medicine) but hadn’t gotten around to it and I guess now I don’t need to. Thanks!
Your bit on the salt/sugar drink reminded me, rather horribly, of my first nightshift at an industrial bakery when I was 18. I was put on the bread roll ovens, which radiated a phenomenal amount of heat, so by my first break, I was desperate for a drink. One of the old lags pointed out a drinks station near the ovens and I gratefully poured myself a generous glass of what I took to be lime cordial. It was, of course, not that simple - being laced with salt to replace what we lost from our profuse sweating. Much to the assembled old lags' delight, I spat the whole mouthful out in horror! It was absolutely vile - even more so because so unexpected. The old boys, some of whom had worked there for decades, drank the stuff as if it was water, but, in the two months I was there, I could never get used to it.